

Modern oncology has entered an era of unprecedented precision, where the goal is no longer just to attack a tumor, but to teach the body’s own immune system to recognize and destroy it. However, this delicate recalibration of the immune response can occasionally open the door to unexpected vulnerabilities, transforming a patient’s fight against cancer into a simultaneous battle with dormant viruses.
A recent clinical case highlights this complexity, detailing a 67-year-old man with metastatic non-minor cell lung cancer (NSCLC) who developed Herpes Zoster—commonly known as shingles—while undergoing a combination of chemotherapy and immunotherapy. The incident underscores a critical challenge for clinicians: balancing the aggressive pursuit of tumor shrinkage with the management of opportunistic infections that emerge when the immune system is suppressed or redirected.
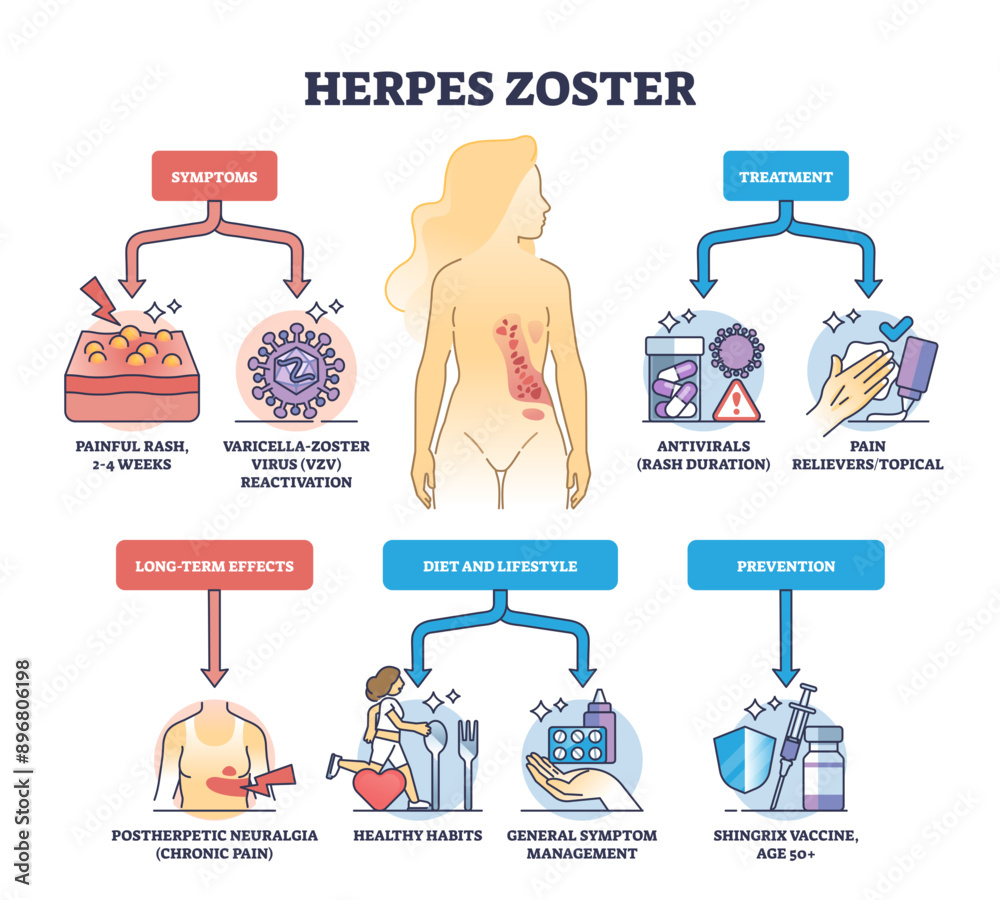
The patient was receiving Pembrolizumab, a programmed cell death protein 1 (PD-1) inhibitor, alongside standard chemotherapy. While this chemo-immunotherapy approach is a cornerstone in treating advanced NSCLC, the synergy of these treatments can create a window of susceptibility. In this instance, the patient presented with a painful, blistering rash localized to the T4 and T5 dermatomes of the chest, a classic sign of the reactivation of the Varicella-Zoster Virus (VZV).
The intersection of immunotherapy and viral reactivation
To understand why Herpes Zoster following Pembrolizumab treatment occurs, it is necessary to look at how these drugs function. Pembrolizumab works by blocking the PD-1 pathway, effectively “taking the brakes off” the T-cells so they can attack cancer cells. While this is the intended goal for tumor regression, the systemic alteration of immune checkpoints can occasionally disrupt the body’s ability to keep latent viruses in check.
When combined with traditional chemotherapy, which reduces the overall count of white blood cells (leukopenia), the patient’s defenses are further lowered. The Varicella-Zoster Virus, which remains dormant in the nerve tissues after a person recovers from chickenpox, takes advantage of this diminished surveillance to travel down the nerve fibers to the skin, resulting in the characteristic painful vesicles of shingles.
For the patient in this case, the onset of the rash was not merely a dermatological issue but a systemic signal. The pain associated with the eruption can be severe, potentially mimicking other complications of lung cancer or immunotherapy-related adverse events, making an accurate and rapid diagnosis essential to prevent long-term nerve pain, known as postherpetic neuralgia.
Comparing immune impacts in cancer therapy
The risk profile for infections differs significantly depending on the type of treatment administered. While chemotherapy provides a broad suppression of the immune system, immunotherapy creates a more targeted, albeit unpredictable, shift in immune activity.
| Treatment Type | Primary Immune Effect | Viral Risk Factor |
|---|---|---|
| Traditional Chemotherapy | General myelosuppression (low WBC count) | Broad susceptibility to opportunistic infections |
| PD-1 Inhibitors (Pembrolizumab) | Checkpoint blockade / T-cell activation | Specific viral reactivations due to immune dysregulation |
| Combination Therapy | Synergistic immunosuppression | Increased risk of rapid viral onset and severity |
Clinical management and recovery
The management of shingles in a patient fighting metastatic cancer requires a dual-track approach: treating the virus without compromising the cancer therapy. In this case, the patient was treated with Acyclovir, a potent antiviral medication designed to inhibit viral replication. Along with pain management protocols, the antiviral therapy helped resolve the skin lesions and prevent the virus from spreading further.
A key aspect of this case was the decision-making regarding the continuation of the oncology regimen. Because the Herpes Zoster infection was managed effectively and did not lead to systemic sepsis or severe organ dysfunction, the patient was able to continue their chemo-immunotherapy. This highlights the importance of “interventional agility”—the ability of a medical team to pivot to treat a secondary infection without abandoning the primary life-saving cancer treatment.
For patients undergoing non-small cell lung cancer treatments, the appearance of a unilateral rash (affecting only one side of the body) should be treated as a red flag. Early administration of antivirals, typically within 72 hours of rash onset, is the gold standard for reducing the duration of the illness and the risk of permanent nerve damage.
Broader implications for oncology care
This case serves as a reminder that the “immune-oncology” landscape is fraught with paradoxes. While we use the immune system to kill the cancer, we must remain vigilant about the “collateral damage” that occurs when the immune system is manipulated. The reactivation of VZV is not an isolated phenomenon; other latent viruses, such as Cytomegalovirus (CMV) or Epstein-Barr Virus (EBV), have also been noted in patients receiving checkpoint inhibitors.
Medical professionals are increasingly advocating for a more holistic monitoring approach. This includes:
- Baseline Screening: Assessing a patient’s history of varicella and their vaccination status before starting immunotherapy.
- Patient Education: Teaching patients and caregivers to recognize the early signs of shingles, such as tingling or burning sensations before the rash appears.
- Proactive Surveillance: Integrating dermatological checks into regular oncology visits to catch skin manifestations of immune dysregulation early.
The ability to treat the cancer while simultaneously managing these side effects is what defines successful modern care. As more patients transition to combination therapies involving Pembrolizumab, the medical community must refine its protocols to ensure that the cure for one disease does not leave the patient defenseless against another.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Patients should consult with their healthcare provider for diagnosis and treatment options regarding cancer therapy and viral infections.
The next step for clinicians will be the integration of more robust prophylactic strategies, potentially including the use of the recombinant zoster vaccine in eligible cancer patients before the initiation of immunotherapy to prevent reactivation entirely. Ongoing clinical trials are currently evaluating the safety and efficacy of such preventative measures in immunocompromised populations.
Do you or a loved one have experience navigating the side effects of immunotherapy? Share your thoughts or questions in the comments below.