

For many, the image of Parkinson’s disease is distilled into a single, visible symptom: the tremor. We see the shorthand the public uses to recognize the condition, a rhythmic shaking of the hand or a shuffling gait that signals a neurological struggle. But for the tens of thousands of people living with the disorder, the tremor is often the least disruptive part of their day.
The true burden of the disease lies in the invisible architecture of the condition—the “non-motor” symptoms that erode a patient’s quality of life long before their movement is severely compromised. From the sudden onset of crushing anxiety to the silent struggle of bladder control and the exhausting cycle of insomnia, the daily challenges of Parkinson’s patients extend far beyond the reach of a visible shake.
In Israel, where approximately 35,000 people are living with the disease, the medical community is working to shift the narrative. While about 6,000 to 7,000 of these patients are in advanced stages requiring significant assistance, the struggle begins much earlier. The disease is a progressive, degenerative neurological disorder that systematically dismantles the brain’s ability to produce dopamine, the chemical messenger responsible for coordinating smooth, purposeful movement and regulating mood, and sleep.
“Parkinson’s affects dopamine production in the brain, and therefore causes motor symptoms such as tremor, stiffness, and slowness of movement,” explains Dr. Michal Cohen, a senior neurologist and specialist in movement disorders at Shaare Zedek Medical Center. Yet, she notes that the motor symptoms are only one side of the coin. “Alongside this, there are too many non-motor symptoms: Sleep disturbances, depression, constipation, problems with bladder control, changes in heart rate, drooling, and difficulty swallowing and speaking. Each patient has a different expression of the disease, and it is very individual.”
The Fragile Window of Relief: Levodopa and the ‘Off’ State
The standard of care for early-stage Parkinson’s typically begins with oral medications, most notably levodopa. This drug acts as a precursor to dopamine, allowing the brain to replenish its depleted stores and significantly restoring function. For many, this period is known as the “honeymoon phase,” where the medication effectively masks the symptoms and allows for a relatively normal existence.
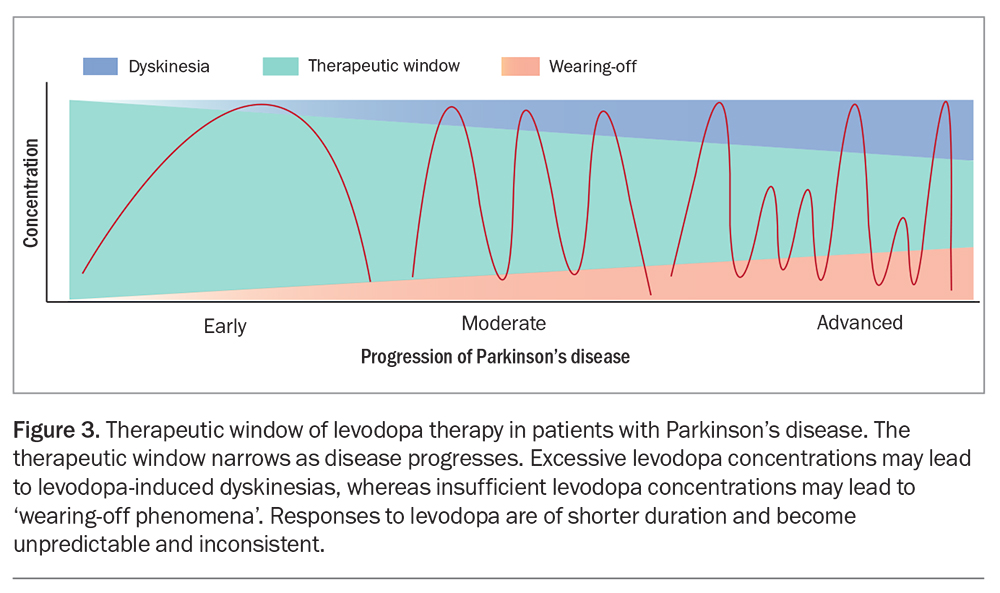
But the efficacy of oral levodopa is often temporary. Over several years, the therapeutic window narrows. The duration of each dose begins to shrink, leading to a phenomenon known as “off states.” During an off state, the medication wears off before the next dose is due, and the patient may suddenly find themselves unable to move—a state of temporary paralysis that is often accompanied by acute anxiety.
When the limitations of oral medication become a barrier to daily living, neurologists look toward more invasive or continuous delivery systems. Deep Brain Stimulation (DBS) is one such option, involving the surgical implantation of electrodes into specific brain regions to regulate abnormal electrical impulses. While DBS can be transformative for motor control, it is not a universal solution; it may not be suitable for patients with certain cognitive impairments, and it often fails to address issues like swallowing difficulties or the “freezing” of gait.
Comparing Modern Parkinson’s Treatment Modalities
As the disease progresses, the goal shifts from simple symptom management to the pursuit of stability. The following table outlines the primary advanced interventions used when oral medication is no longer sufficient.
| Treatment Method | Delivery Mechanism | Primary Benefit | Key Constraint |
|---|---|---|---|
| DBS Surgery | Implanted Electrodes | Significant motor control | Invasive; not for all cognitive profiles |
| Intestinal Pump | Direct Digestive Infusion | Stable medication levels | Requires permanent invasive device |
| Subcutaneous Pump | Under-skin Patch/Tube | 24-hour continuous delivery | Requires patch replacement every 48h |
A more recent evolution in care is the subcutaneous pump. Unlike the intestinal pump, which requires a more invasive surgical procedure, the subcutaneous pump delivers levodopa continuously through a thin, flexible tube inserted under the skin, similar to an insulin pump. This method more closely mimics the body’s natural physiological state by maintaining a steady level of the drug in the bloodstream, reducing the sharp “peaks and valleys” associated with pills.
“The main advantage is continuity,” Dr. Cohen says. “Instead of a short effect from a pill, there is a more stable level of the drug in the blood. This allows better control of motor symptoms throughout the day and also at night.”
The Nightly Battle: When Sleep Becomes a Symptom
While the world sees the patient during the day, the most grueling challenges often emerge after the lights go out. Sleep disturbances are among the most pervasive yet under-discussed aspects of the disease. Stiffness makes it nearly impossible for patients to turn over in bed, and frequent awakenings lead to a state of chronic daytime fatigue.
The impact is not limited to the patient. Approximately 90% of Parkinson’s patients suffer from these sleep disruptions, and nearly 90% of their caregivers report that their own sleep is similarly affected. This creates a cycle of exhaustion that can strain the emotional bond between partners and increase the risk of falls when a patient attempts to get up in the middle of the night.
The introduction of continuous delivery systems has provided a breakthrough in this area. When medication remains active through the night, patients are less likely to feel “stuck” in bed. “Sleep improves, and this has a dramatic impact on quality of life, both for the patient and for the person caring for them,” Dr. Cohen notes.
The Path Forward: Specialized Care and Movement
As independence wanes, the role of the caregiver becomes central. Managing a complex regimen of medications and coping with the emotional volatility of the disease can be an overwhelming burden. Because the field of movement disorders is evolving so rapidly, many patients are not aware of the latest options. General practitioners may not always be current on the newest pump technologies or the specific criteria for specialized clinic referrals.
Neurologists emphasize that when initial treatments cease to be effective, a referral to a specialized movement disorders clinic is essential. These centers not only provide personalized treatment plans but also offer access to clinical trials that may provide the next leap in care.
Amidst the high-tech interventions, one of the most powerful tools remains the most basic: physical activity. While it may seem paradoxical to push for movement in a disease that inhibits it, exercise is critical for maintaining neural plasticity and muscle function. “Physical activity is one of the most crucial tools for maintaining function,” Dr. Cohen concludes.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
The medical community continues to refine the balance between pharmacological stability and surgical intervention. The next critical checkpoints in Parkinson’s care will likely involve more refined “smart” delivery systems and a deeper understanding of the non-motor triggers that affect sleep and mood. By addressing the invisible symptoms, the goal is to ensure that patients do not just survive the disease, but maintain a meaningful quality of life.
Do you or a loved one navigate the challenges of Parkinson’s? We invite you to share your experiences and insights in the comments below.