

For millions of people living with diabetes, the risk of vision loss is a constant, quiet concern. Whereas the biological mechanisms of diabetic eye disease are well-documented, a growing body of research reveals that the path toward treatment-warranted diabetic eye disease is not the same for everyone. A combination of racial and microvascular determinants—ranging from genetic predispositions to systemic barriers in healthcare access—creates a stark disparity in who loses their sight and how quickly it happens.
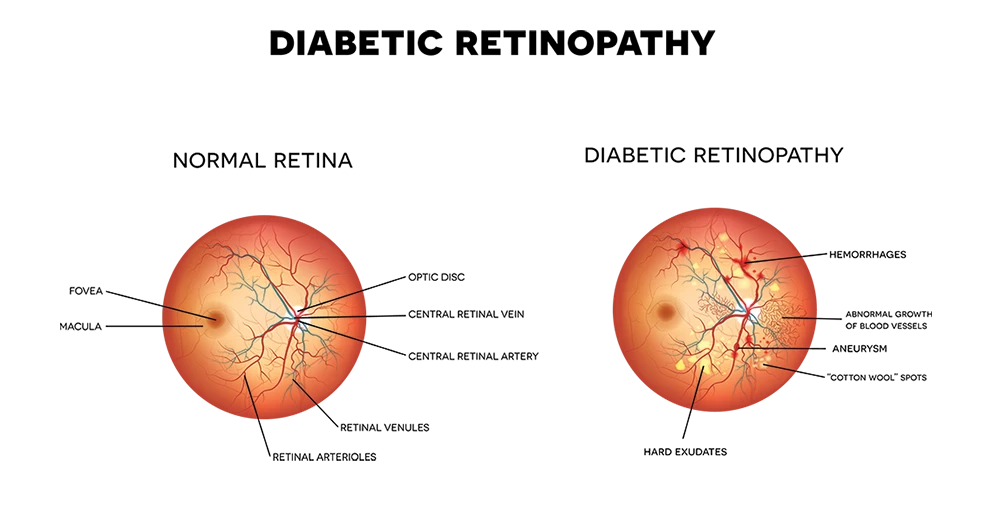
Diabetic retinopathy, the primary driver of this vision loss, occurs when high blood sugar levels damage the tiny blood vessels in the retina. When these vessels leak or close, the eye may attempt to grow new, fragile vessels that can bleed and cause severe impairment. However, the progression from early stages to a state requiring medical intervention is heavily influenced by a patient’s ethnic background and the health of their other microvascular systems, such as the kidneys.
Recent data underscores a troubling trend: marginalized populations often face a “double burden.” They are not only more likely to develop sight-threatening complications but are also less likely to receive the timely screenings necessary to prevent them. This intersection of biological vulnerability and social inequality means that for many, the first sign of eye disease is a sudden, irreversible drop in vision rather than a manageable diagnosis during a routine checkup.
The Biological and Racial Divide in Vision Loss
Research indicates that ethnicity plays a significant role in the prevalence and speed of retinopathy progression. For instance, studies have shown a higher prevalence of retinopathy in patients of South Asian ethnicity compared to White Europeans in community settings. Similarly, American Indian and Alaska Native populations have shown distinct patterns of incidence and progression, often exacerbated by a higher baseline of other comorbidities.
These disparities are not merely about the presence of the disease, but the rate at which it evolves. Some populations experience a more aggressive transition to proliferative diabetic retinopathy—the stage where new blood vessels grow—which necessitates urgent treatment to avoid permanent blindness. This biological variance suggests that a “one size fits all” screening interval may be insufficient for high-risk ethnic groups.
Beyond genetics, the health of the microvascular system as a whole serves as a critical predictor. There is a strong correlation between diabetic retinopathy and diabetic nephropathy (kidney disease). When the microvascular determinants in the kidneys fail, it often signals a systemic vulnerability that accelerates the deterioration of the vessels in the eyes. For patients with declining renal function, the risk of rapid progression to treatment-warranted eye disease increases significantly.
Systemic Barriers and the ‘Treatment Gap’
While biological factors are influential, the “treatment-warranted” aspect of eye disease is often determined by when a patient first enters the clinic. In the United States, racial disparities in the timing and frequency of eye examinations are well-documented. Working-age populations of color often face greater hurdles in accessing the specialized care required to manage retinopathy before it becomes sight-threatening.
These barriers are often rooted in social determinants of health, including insurance status, geographic location, and the availability of transportation. Patients in rural areas or those relying on underfunded community clinics may wait longer for a referral to an ophthalmologist, allowing a treatable condition to progress into a crisis. This delay transforms a manageable medical issue into a disability.
The impact extends beyond the eyes. There is a documented link between the severity of diabetic eye disease and other microvascular complications, such as diabetic foot ulcers. Patients who struggle to access eye care often face similar systemic failures in foot care, leading to higher rates of lower-extremity amputations among specific racial and ethnic groups. This suggests that the “treatment gap” is a systemic failure of integrated care rather than a failure of individual patient compliance.
Comparative Risk Factors and Outcomes
| Determinant Type | Key Factors | Impact on Progression |
|---|---|---|
| Microvascular | Renal dysfunction / Nephropathy | Accelerates retinal vessel damage |
| Racial/Ethnic | South Asian, Indigenous/Native groups | Higher prevalence and faster progression |
| Systemic | Lack of routine screenings | Delayed diagnosis until sight-threatening |
| Clinical | Uncontrolled blood glucose/BP | Increases risk of proliferative stages |
The Role of Modern Therapeutics and Screening
The introduction of new pharmacological treatments, including GLP-1 receptor agonists like semaglutide, has added a new layer of complexity to the management of diabetic eye disease. While these medications are highly effective for glycemic control and weight loss, some research has explored their association with the risk of retinopathy. Understanding how these drugs interact with the existing microvascular determinants of different racial groups is a current priority for clinicians.
To bridge the disparity gap, public health experts are advocating for a shift toward “precision screening.” This approach would use a patient’s racial background and other microvascular markers—such as kidney function tests—to determine how often they should be screened. By increasing the frequency of exams for those at the highest biological and social risk, providers can catch the disease in the non-proliferative stage, where simple blood pressure and glucose management can often halt progression.
the integration of AI-driven screening tools in primary care settings is seen as a way to bypass some of the systemic barriers. By allowing a primary care physician to perform an initial retinal scan and use software to detect early signs of disease, the “referral lag” that currently plagues marginalized communities could be significantly reduced.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult a board-certified healthcare provider for diagnosis and treatment of diabetic eye disease.
The next critical step in addressing these disparities will be the implementation of updated Standards of Care in Diabetes, which continue to refine the guidelines for retinopathy, neuropathy, and foot care to better account for diverse patient populations. As these guidelines evolve, the focus is expected to shift toward more aggressive, personalized screening protocols for high-risk groups.
We invite you to share your experiences with diabetes management and eye care in the comments below. How has access to screening impacted your health journey?